Patient Resources
Your Elbow
Anatomy of the Elbow
 The elbow is a hinge joint made up of the humerus, ulna and radius.
The elbow is a hinge joint made up of the humerus, ulna and radius.
The unique positioning and interaction of the bones in
the joint allows for a small amount of rotation as well
as hinge action. This rotation is easily noticed during
activities such as hand-to-mouth eating motions.
The primary stability of the elbow is provided by the
ulnar collateral ligament, on the medial (inner) side of
the elbow.
However, one of the most common injuries to the
elbow occurs on the lateral, or outer, side of the elbow — it is called "lateral epicondylitis" or "tennis elbow."
Tennis Elbow
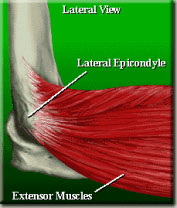 Tennis elbow, or lateral epicondylitis, is one of the most common elbow
problems seen by an orthopedic surgeon. It is actually a tendinitis of the
muscle called the extensor carpi radialis brevis, which attaches to the
lateral epicondyle of the humerus.
Tennis elbow, or lateral epicondylitis, is one of the most common elbow
problems seen by an orthopedic surgeon. It is actually a tendinitis of the
muscle called the extensor carpi radialis brevis, which attaches to the
lateral epicondyle of the humerus.
It may be caused by a sudden injury or by repetitive use of the arm.
Many doctors feel that micro tears in the tendon lead to a hyper-vascular
phenomenon resulting in pain. The pain is usually worse with strong
gripping with the elbow in an extended position, as in a tennis back hand
stroke, but this problem can occur in golf and other sports as well as with
repetitive use of tools.
Before surgery is considered a trial of at least six months of conservative
treatment is indicated and consists of a properly placed forearm brace
and modification of elbow activities. I have not found anti-inflammatory medication or physical therapy to be of
any value. If the above treatment is not helpful, a cortisone injection can be beneficial but no more than three
injections are recommended in any one location in a year.
Conservative treatment is in two phases and after Phase I (Pain relief) has been successful, Phase II,
(Prevention of recurrence) is equally as important and involves stretching and then later strengthening
exercises, so the micro tears will not occur in the future.
When conservative treatment has failed, then surgery is indicated. Many procedures have been described.
Procedures as simple as percutaneous release of the tendon off of the bone have been described and more
recently arthroscopic procedures or other procedures involving the joint and resection of a ligament as well
have been described.
The most popular procedure today is a simple excision of diseased tissue from within the tendon, shaving
down the bone and re-attachment of the tendon. This can be performed as an outpatient procedure
with regional anesthesia (where only the arm goes to sleep) and through a relatively small incision of
approximately 3″ long. 85-90% of patients with this technique are typically able to perform full activities
without pain after a recuperation of two to three months. Approximately 10-12% of patients have improvement
but with some pain during aggressive activities and only 2-3% of patients have no improvement.
Golfers Elbow
Medial epicondylitis is inflammation of the tendon attachment of the flexor pronator muscles in the forearm.
Usually this begins as microscopic tears in the tissue, which leads to an inflammatory or hypervascular
process. This occurs when stiff, underused tendons are suddenly overused or this may occur from an acute
injury.
The treatment includes three treatment options, no treatment, conservative and surgery.
Surgery is a last resort and involves cleaning up the tendon from diseased tissue, shaving down the bone and
re-attachment of the tendon. This is necessary in 10-15% of the patients.
Conservative treatment is in two phases, Phase I is to get rid of the pain and Phase II is to prevent it from
coming back with stretching and strengthening exercises. To reduce the pain, using the elbow in a flexed
position and the use of an elbow strap counterforce brace is usually the first line of treatment. If the patient
has persistent symptoms a cortisone injection may be considered. No more than three injections are
recommended per year and if the patient still has persistent symptoms despite conservative treatment surgery
is considered.
Cubital Tunnel Syndrome
Cubital tunnel syndrome is a pinched nerve at the elbow commonly known as the "funny bone." This might
be caused by trauma or repetitive use of the elbow and may be caused by continuous use of the elbow in
a flexed position. This causes the nerve to become stretched and irritated as opposed to when the arm is
extended and the nerve is in a relaxed position. The diagnosis can be confirmed with electrodiagnostic testing
including nerve conduction velocity and the electromyogram. Nerve conduction velocity studies, the speed of
the nerve across the elbow, will be slowed when there is nerve compression and electromyogram studies, the
innervation of the muscles, might be affected by the pinched nerve.
For this problem there are three modes of treatment - no treatment, conservative and surgical. Unfortunately
with conservative treatment, only splinting with the arm in an extended position has been found to be helpful.
Cortisone injection, physical therapy, and anti-inflammatory medications, have not been seen as beneficial.
Nighttime splinting is achieved with a custom made long arm splint that the patient will wear at nighttime and
as often as possible during the day. Unfortunately it is cumbersome to keep the arm out straight all the time
and therefore this is usually used only at night. If the patient has persistent complaints despite conservative
treatment surgery would be recommended. There are three types of procedures, one is to cut the medial
epicondyle which is the bone pinching the nerve or the other two operations are to actually move the nerve
out of the cubital tunnel either above or below the muscles of the forearm. This can be performed as an
outpatient procedure with an axillary block where only the arm is put to sleep and it has a high success rate.
|
For Our Patients
Existing patients may utilize these convenient links to access forms, educational materials and manage their accounts.
Medical Questionnaire
Patient Forms
Convenient, Online
Patient Forms Are
Coming Soon!
Pay My Bill
INSURANCE PROVIDERS WE PARTICIPATE WITH:
Commercial
Blue Cross/Blue Shield
DMBA
HMA
HMAA
HMSA PPO & HMSA HMO
MDX
UHA
Government
Medicare
Medicaid
OHANA/Wellcare
Triwest/Tricare
UHC- Medicare Advantage
Other
Workers Compensation
No-Fault
|